CBBLE UDHC SIMILAR CASES
"This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current based inputs.
Unit 3 & 6
Amc bed 5
Chief complaints:
Patient came to casualty with complaints of pain in abdomen from today morning
History of presenting illness:
55yr/M barber by occupation was apparently asymptomatic 15 years back then he had c/o pain abdomen diagnosed as intestinal perforation discharged after 1 week and again he complains of abdominal pain since today morning which was in midline between epigastric and umbilicus squeezing type sudden in onset progressive, aggravates on deep inspiration and no radiation not associated with nausea and vomiting.also have c/o chest pain , epigastric region burning type not associated with palpitations and syncopal attacks
No c/o sob,asthma,pnd
Past history:
Not a known case of htn/dm/cad/tb/ bronchial asthma
Surgical history: previously had surgery for intestinal perforation.
Personal history:
Married
Barber by occupation
Diet:mixed
Appetite:normal
Bowel bladder movements: regular
Addictions: alcohol consumption since 25 years
90-180ml whiskey per day
Family history: not significant
O/e:
Pt is conscious,coherent and cooperative well oriented to time,place,person
No signs of pallor,icterus,clubbing,cyanosis,lymphadenopathy,pedal edema.
Vitals:
Temp:afebrile
Pr:98bpm
Rr:18cpm
Bp:140/100
Spo2:98%
Grbs:165mg/dl
Systemic examination:
Cvs: S1,S2 heard,no murmurs heard
Rs:BAE +,NVBS heard
P/A: scar present on the epigastric region,soft,tenderness present in epigastric region. Mild Rigidity present in the epigastric region.
Bowel sounds present
Cns: NAD
Diagnosis:acute pancreatitis
Clinical images:



Investigations:
LFT
TB:2.18
DB:0.79
AST:51
ALT:27
ALP:176
TP:7.5
ALB:4.5
RFT
Urea:20
Creatinine:0.9
Na:139
K:3.2
CL:103
S.amylase:579.4
Hemogram:

Cxr:

X ray erect abdomen:

ECG:

Ultrasound abdomen:
Pancreas shows altered echotexture with surface irregularity
Evidence of peripancreatic fluid collection
Mild ascites
Grade 1 fatty liver
CT scan abdomen:
Pancreas is edematous with significant peripancreatic and mesentric fat stranding.
Plan:
1.Ivf with ns and rl at 125ml/hr
2.NBM till further order
3.Inj pan 40mg/iv/bd
4.inj zofer 4mg/iv/bd
5.inj tramadol 1amp in 100ml Ns/iv/tid
6.inj optineuron 1amp in 100ml ns/iv/od
7.inj thiamine 1amp in 100ml ns/iv/tid
8.strict input output charting
Surgery referral:
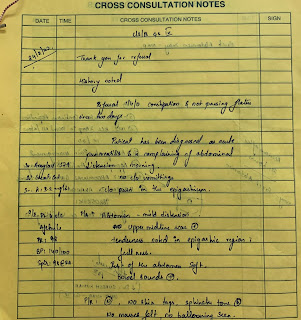





This is peripancreatic fat stranding secondary to acute pancreatitis.
Soap notes
Day 1
S: no fever spikes since yesterday
Pain subsided
O:
O/e
Patient is c/c/c
Temp:99.6
Pr:110bpm
Rr:18cpm
Bp:140/100
Spo2:98% at RA
Cvs: S1 S2 +, no murmurs
Rs: BAE +
PA: soft,tender
GRBS: 141mg/dl
A: acute pancreatitis
P:
1.ivf with ns and rl at 125ml/hr
2.NBM till further order
3.inj pan 40mg/iv/bd
4.inj zofer 4mg/iv/bd
5.inj tramadol 1amp in 100ml ns/iv/tid
6.inj optineuron 1am in 100ml ns/iv/od
7.inj thiamine 1amp in 100 mlns/iv/tid
8.strict input output charting
Soap notes
Day 2
55yr/M
S: no fever spikes since yesterday
Pain subsided
O:
O/e
Patient is c/c/c
Temp:afebrile
Pr:110bpm
Rr:18cpm
Bp:170/100
Spo2:98% at RA
Cvs: S1 S2 +, no murmurs
Rs: BAE +
PA: soft,non tender
GRBS: 122mg/dl
A: acute pancreatitis
P:
1.ivf with ns and rl at 125ml/hr
2.NBM till further order
3.inj pan 40mg/iv/bd
4.inj zofer 4mg/iv/bd
5.inj tramadol 1amp in 100ml ns sos
7.inj thiamine 1amp in 100 ml ns/iv/tid
8.strict input output charting


Comments
Post a Comment